
Review Article | DOI: https://doi.org/10.31579/2690-8794/031
1 Laboratoire de Physiologie Intégrée, Faculté des Sciences de Bizerte, Université de Carthage, Jarzouna, Tunisia.
2 Laboratoire de Valoristaion des Bio-Géo-Resources, Ecole Nationale de Médecine Vétérinaire de Sidi Thabet, Université de la Manouba, Sidi Thabet, Tunisia.
3 Laboratoire de Physiologie Intégrée, Université de Carthage, Faculté des Sciences de Bizerte, Jarzouna, Tunisia.
*Corresponding Author: Amel Hanini, PhD,Laboratoire de Physiologie Intégrée, Université de Carthage, Faculté des Sciences de Bizerte, Jarzouna, Tunisia.
Citation: Abdelmelek H., Souilem O. and Hanini A., (2020) Nanotoxicity of corona-nanoparticles (SARS-COV-2): Nanomechanisms of hypoxia J, Clinical Medical Reviews and Reports. 2(5);DOI:10.31579/2690-8794/031
Copyright: © 2020 Amel Hanini, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 25 June 2020 | Accepted: 10 July 2019 | Published: 08 September 2020
Keywords: SARS-COV-2; covid-19; monge disease; chloroquine; nanotoxicity
The present review aim to help scientific community to better understand, in vitro and in vivo, COVID-19 compared to Monge disease (MD). The SARS-COV-2 or Corona-nanoparticles (NPs: 60-140nm) model based on nanosciences give an innovative understanding of virus nanotoxicity associated to violent inflammatory reactions and acute respiratory distress. Our analysis of COVID-19 suggest for the first time as far as we know that SARS-COV-2 use nanosciences laws such as virus agglomeration and mitochondria respiration toxicity induced by cluster virus-Heme. Moreover, the implication of age, gender, and ethnicity to COVID-19 must be confirmed by future studies compared to MD. Virus could use nanomechanisms to induce hypoxia via generation of Heme-virus clusters mitigating microcoagulation implicated in acute respiratory distress and heart failure. Our analysis point to the presence of possible link between hypoxia and COVID-19 pro-pulmonary complications.
Until now in the field of virology and nanomedicine, viral diseases related to COVID-19 (Coronavirus disease 2019) can be considered as a mystery to their unusual mechanism of pathogenicity. Take anything you learned in the field of epidemiology, especially about recent
viral diseases and throw it out the door because COVID-19 are exceptional and probably the only pathology with this exceptional physiopathology and leading to important lethality (Carlo et al, 2020). Recently, huge controversy related to the use of different drugs such as Hydroxychloroquine and Chloroquine (Dogar et al, 2018) against COVID-19. In the absence of specific COVID-19 treatment or vaccination, this drug protocol is the most hotly discussed issues in molecular-cellular toxicity and therapeutic of these molecules (Cascella et al, 2020). For all these considerations we propose a new interpretation based on nanosciences, physiology, physiopathology, and nano-pharmacology on SARS-COV-2 cytopthogeny as nanoparticles (NPs). NPs cytotoxicities are related to several physicochemical properties such as concentration, size, up-take mechanism (Hanini et al, 2011). The toxicity of Co-ferrite oxide NPs may be attributed either to their direct uptake by cells or to their dissolution leading to the increased level of cationic ions in the growth media and/or inside the cells. Focusing on cobalt-ferrite NPs, literature remains controversial where some findings shows in vitro and in vivo toxicities and others found that Co- Superparamagnetic Iron Oxide Nanoparticles (SPIONs) are not cytotoxic. Different types of SPIONs, varying in their composition and/or surface coating, can be synthesized, depending on the requirements for their application (Mahmoudi et al., 2009; Baratli et al., 2013).
Properties of Corona-nanoparticles (SARS-COV-2)
The present review provides a detail overview of NPs properties. NPs are tiny materials having size ranges from 1 to 100nm such as Covid-19 having a diameter of approximately 60–140 nm (Cascella et al, 2020). Recently in 2020, the structure of the virus in the cytoplasm of three day post-inoculation cells was examined by electron microscopy; showing that virus particle size ranged from 70–90 nm and the virus was observed in a wide range of intracellular organelles, especially in vesicles (Jeong-Min et al, 2020). Coronaviruses are enveloped and have single stranded positive sense RNA genomes. A coronavirus particle consists of four structural proteins: the nucleocapsid, envelope, membrane and spike. The Spike (S) protein (about 20nm) forms club-shaped protrusions that stick out all over the virion, resembling a crown or the sun’s corona.
Transmission of virus is usually via airborne droplets (>5000nm) to the nasal mucosa and contaminated surfaces. SARS-CoV-2 attacks human angiotensin converting enzyme 2 (ACE-2) in numerous tissues especially ciliated bronchial, epithelial cells and type II pneumocytes. Moreover, SARS-CoV-2 infection induces atypical pneumonia associated to high levels of pro-inflammatory cytokines. SARS-COV-2 NPs possess unique physical and chemical properties due to their high surface (S) area compared to volume (V) (S/V ratio) and nanoscale size directly or indirectly implicated in different biological process such as inflammation independently of classic
immunological reactions. Interestingly, nanotechnology could be developed in physico-chemistry Labs or in living systems (Bottom-up approaches) as viral replication in cells by bioengineering nanomechanisms.
Nanotoxicology have demonstrated that physic-chemical properties of NPs including size, shape, surface coating, surface charge, solubility, and chemical composition could dramatically affect Corona-NPs behaviour in biological systems and thus modulate Human and Animal toxicity in blood and tissues. In nanosciences, the uncoated-NPs (U-NPs) agglomerate with chemical and physical laws in the environment and organs (Hanini et al, 2011, Ferchichi et al, 2016). The investigation of the physico-chemical characteristics and their impact on the biological effects of Corona-NPs is important to better understanding their pneumotoxic mechanism. We discuss a new model based on the concept of induction of COVID-19 by a simple conversion of uncoated SARS-COV-2 or corona-NPs (U-NPs) to coated NPs (C-NPs), which is a normal form of virus implicated in the bioengineering of the virus known as viral cycle. The U-NPs (SARS-COV-2) agglomerate with chemical and physical In addition, drug (such as Hydroxychloroquine and Chloroquine) are proposed to be used for COVID-19 therapy but the mechanism of action of this drug against SARS-COV-2 is still unknown. Both drugs have a flat aromatic core structure at nano-scale levels. The basic side chain is thought to contribute to the accumulation of these drugs in intracellular compartments, especially lysosomal compartments. Interestingly, the anti-inflammatory effects of hydroxychloroquine and chloroquine could be explained by the inhibition of lysosomal activity.
A key pathological feature of SARS-Cov-2 NPs is hypoxia that could be analyzed or compared to pseudo-Monge disease. Hypoxia can be considered as a failure of oxygen supply to maintain tissue ATP production. The normal alveolar Po2 (∼ 110 mm Hg) is high than other organs in which oxygen tension ranges from 3–20 mm Hg (Monge et al., 1989).
Acute respiratory distress is a severe form of hypoxic diseases responsible for a large number of deaths worldwide induced by SARS-COV-2. New strategies are urgently required to help scientist to understand SARS-Cov-2 nanotoxicity and to design innovative therapies. We will review recent advances in our understanding of COVID-19 disease and the physiopathology of direct or indirect hypoxia. The direct hypoxia is related to alveolar alteration of oxygen supply and indirect hypoxia is linked to disruption of oxygen transport via erythrocytes. Comparative physiology or physiopathology of acute respiratory distress between COVID-19 to Monge Disease may provide new insights into the implication of nanomechanisms of cellular interactions between erythrocyte
(70000 nm) and virus (60-140nm). Hypoxia in COVID-19 as in Monge Disease induced organ ischemia and inflammatory process (Monge et al., 1989). In both diseases, the hypoxia-induced inflammatory response results in the recruitment of immune cells, the activation of downstream signaling pathways, and the induction of pro-inflammatory cytokines and chemokines. In addition, these extremely low concentrations of oxygen prolong neutrophil survival and increase endothelial permeability and vascular leakage. Interestingly, the mechanisms of hypoxic responses have been extensively investigated in animal models in vivo, where hypoxic–ischemic conditions are typically induced by vascular occlusion, and in vitro models in which oxygen has been reduced to 0.5–1.0%, mimicking the oxygen concentrations encountered during ischemia. The first to be identified was the hypoxia-inducible factor (HIF) family, which responds in a rapid manner to profound reductions in cellular oxygen concentration (Monge et al., 1989).
At high altitude, hypertension induces right heart failure and death in susceptible individuals, as seen in Monge disease. Moderate alveolar hypoxia, high altitude, provokes an increase of macrophages, neutrophils, and inflammatory cytokines, including IL-1β, IL-6, IL-8, and TNF-α, in human bronchoalveolar lavage fluid. Similarly, rodents exposed to alveolar hypoxia demonstrate a pulmonary infiltration of neutrophils, macrophage associated to increased pulmonary vascular permeability and elevations of inflammatory cytokines in lung. The comparative physiopathology of hypoxia demonstrates in human and animal inflammatory pulmonary lesions (Monge et al., 1989).
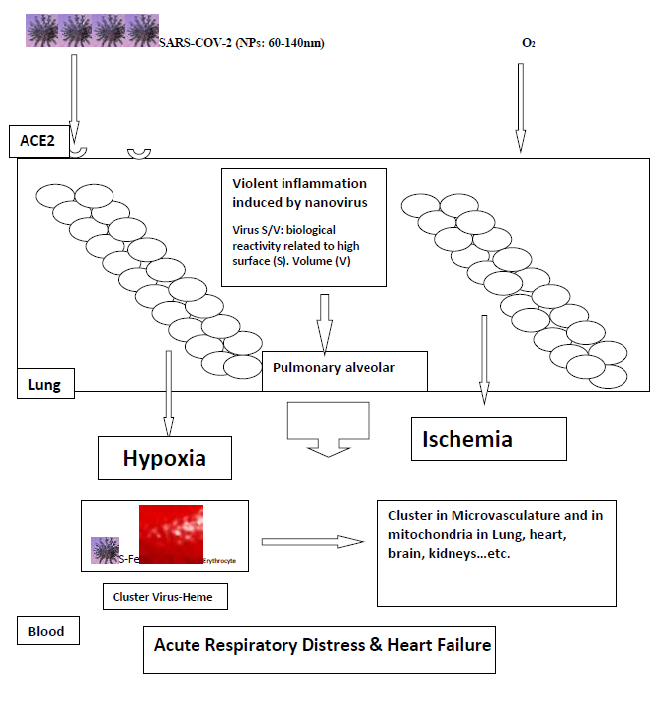
The SARS-COV-2 as nanoparticles could induce mitochondria toxicity indirectly induced by iron released from Heme or a different cluster Fe-S between virus and Heme activating Fenton reaction (Figure 1). Interestingly, mitochondria are considered a major cell compartment relevant to possible SARS-COV-2nanoparticle toxicity. Impairment of mitochondria might be a key problem since mitochondrial dysfunction may result in reduced cellular ATP delivery, increased reactive oxygen species production, and triggering of apoptosis pathways. Accordingly, mitochondrial dysfunctions occur early in many acute or chronic diseases such as peripheral arterial or pulmonary diseases. Mitochondrial involvement in SPIONs toxicity remains controversial and either no deleterious effects or mitochondrial impairments have been observed. Baratli et al (2014) reported that age-dependent accumulation of mitochondrial iron or other nanoparticules (like cluster Heme Fe-S: virus) may increase mitochondrial dysfunction and oxidative damage, thereby enhancing the susceptibility to apoptosis. Therefore, age might modify the susceptibility of mitochondria to iron nanoparticles (NPs). Since, to date, few studies investigated the potential effects of iron oxide nanoparticles on middle-aged mitochondria. Our previous investigation compared the effects of three different concentrations of Fe3O4 nanoparticles
(250, 300, and 350 μg/mL) on young and middle-aged liver mitochondrial respiratory chain complexes activities and on mitochondrial coupling of phosphorylation to oxidation, showing that, unlike young animals, middle-aged rats are sensitive to iron oxide nanoparticles. Indeed, liver mitochondrial respiration chain complexes I, II, III, and IV activities are altered by Fe3O4 NPs. Further, 250, 300, and 350 μg/mL of Fe3O4 specifically impair liver mitochondrial coupling in middle-aged rats. The fragility of mitochondria seems to increase in function of age. In addition, aging induces loss of mitochondrial function in rodents and monkeys. In mitochondria, the iron complex probably induced Fenton reaction with endogenous H2O2 to produce the highly reactive ˙OH radical. Meanwhile, the continuous production of ˙OH is toxic to cells because it depolarizes the mitochondrial membrane potential, blocking the cell cycle in different organs such as lung, heart, kidneys, and brain (Baratli et al, 2014). These results establish a new system for Fe-mediated ˙OH generation via intra-mitochondrial Fenton reaction in response to the microenvironment of hypoxia in different tissues, which opens a promising research and therapeutic roots against COVID-19. In COVID-19, some patients probably develop severe hypoxemia due to evident nanocluster virus-Heme interaction and trigger excessive erythrocyte production associated to high level of hemoglobin and hematocrit (Figure 1).
COVID-19 could be considered in part as Pseudo-Monge Disease
Monge's disease (MD) is a progressive incapacitating syndrome caused by long term exposure to hypoxia. MD is characterized by severe erythrocytosis (SE; women hemoglobin Hb ≥19 g/dL, men Hb ≥21 g/dL) inducing hypoxia and pulmonary hypertension leading to cor-pulmonale and congestive heart failure. In sum, there is a need for appropriate and innovative medical information and interpretations of hypoxic diseases in order to provide adequate physiopathology mechanisms of COVID-19.
The purpose of this analysis is to address comparative physiopathology and nano mechanisms of hypoxia in MD and COVID-19. In altitude, Human physiology hypoxia is known as a deviation above the mean Hb concentration (Monge et al., 1989). Interestingly, recent study by Cao et al (2020) point that ACE2 expression analysis in lung tissues from Asian and Caucasian populations are still controversial. Moreover, molecular analysis of single-cell RNA-sequences revealed that the Asian donor had higher ACE2 expression cell ratio than African-American and white donors. In addition, the physiological adaptation of people to altitude and hypoxia was different betweenwomen and men. In the same way, native Ethiopians are more adapted than Andeans and Han immigrants (Moore, 2001). This adaptation is reflected essentially in a lower Hb concentration, and therefore in a lower prevalence of SE and MD. While, the lowest values are found in Tibetans (Qinghai-China) with a MD prevalence of about 1.21%; compared to Han immigrants (5.60%) in the same city (Wu et al., 1998). In the Andes, the highest values of prevalence were about 15.40% in men (30-39 years) and increased until 33% (about 60 years) (Monge et al., 1989).
Interestingly, acute respiratory distress and a large number of deaths induced by altitude or SARS-COV-2 are the most important facts of MD and COVID-19. These observations must be validated in COVID-19 patients from different age, gender, and ethnics as previously demonstrated in MD. At a similar altitude and using the same diagnostic criteria, this variability could be attributed mainly to differences in ethnicity. People living longer time at high altitude probably is more likely to be better adapted to hypoxia. The question is whether people living at high altitude react to COVID-19 and by the way we can explain the discrepancy of death recently reported in USA with COVID-19 black patients compared to other American citizens (Figure 1).
Taken together, scientist must compare different symptoms in COVID-19 with MD. The most important symptoms observed in MD are sleep disturbances, headache, lack of mental concentration, loss of appetite, fatigue, breathlessness and/or palpitations, localized cyanosis, dilatation of veins, and muscle and joint pain. In addition, in MD radiographic examination reveals right-ventricular hypertrophy. Interestingly, autopsy of MD patients reported generalized brain and visceral congestion (Peñaloza et al., 1971).
The most important MD symptom is the loss of human or animal ventilatory acclimatization to altitude (Leon-Velarde and Richalet, 2006) and recently observed in COVID-19. Evidence at different levels suggests a genetic basis for SE associated to age, gender, ethnicity, and pathologies such as obesity that could enhance directly or indirectly tissues inflammations. In MD and probably in COVID-19, the lack of respiratory sensitivity to hypoxia and hypoventilation is observed in advanced age, male gender, and overweight are all risk factors (Leon-Velarde et al., 2005).
In this context, several pharmacological approaches have shown promising results in the treatment of SE and MD such as ACE inhibitors (Plata et al., 2002), dopaminergic antagonists, acetazolamide and ventilatory stimulants (medroxyprogesterone) (Kryger et al., 1978) and almitrine (Villena et al., 1985). Thus, we propose COVID-19 treatment based on acetazolamide.
Our analysis of COVID-19 suggest for the first time as far as we know that SARS-COV-2 as nanoparticles inducing agglomeration, violent inflammation, and mitochondria respiration toxicity. Moreover, SARS-COV-2 provokes many similar symptoms previously observed in MD such as acute respiratory distress. The implication of age, gender, overweight and ethnicity to COVID-19 must be confirmed by future studies compared to MD. Virus could use nanomechanisms to induce hypoxia via generation of Heme-virus clusters mitigating microcoagulation. The most important question is whether patient living at high altitude and adapted to hypoxia will have different nanomechanisms against SARS-COV-2 compared to normoxic patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
